
By Ashleigh Elkins
Background
A thyroglossal duct cyst is a congenital abnormality that results from a persistent thyroglossal duct. Thyroglossal cysts present as a neck swelling, generally in the midline or slightly to one side. They are generally smooth and painless. However, thyroglossal cysts are prone to infection and an infected cyst will often be quite painful.[1] Some patients may also experience other symptoms related to the cyst, including dysphagia and hoarseness.[2] Approximately 2/3 of patients with thyroglossal cysts have ectopic thyroid tissue within the cyst.[1]
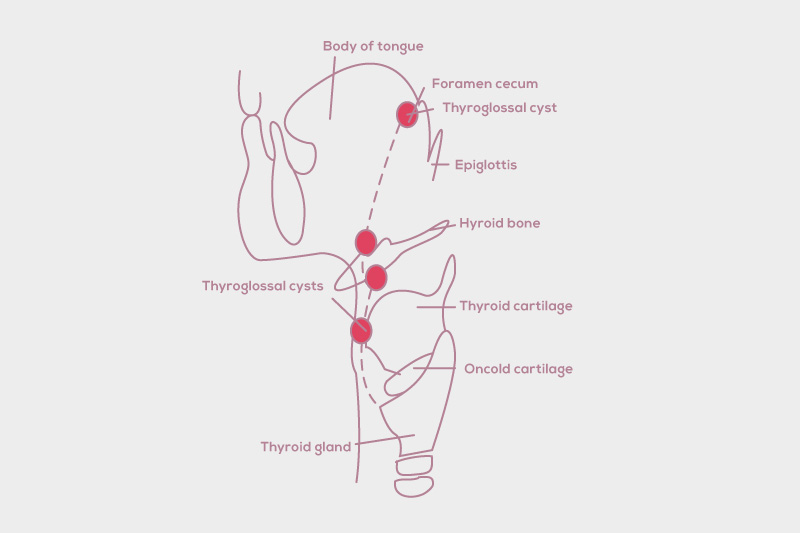
Upon physical examination, a thyroglossal cyst can be differentiated from other neck lumps by observing the movement of the cyst/lump when the patient is swallowing or protruding their tongue. If the lump is a thyroglossal cyst, it will move upwards with swallowing or tongue protrusion.[1] The majority of thyroglossal cysts are detected during childhood. The location of a thyroglossal duct cyst can vary. Some are located above the hyoid bone, others are between the hyoid bone and thyroid cartilage and others are below the sternum. Cysts may also occur within the tongue.[2] The majority of thyroglossal cysts are located below the level of the hyoid bone, with approximately 60-80% of thyroglossal cysts being infrahyoid.[1]
Embryology
The thyroid gland initially develops on the base of the tongue and migrates to its final anatomical position during later stages of development. At approximately gestational week four, the foramen cecum develops as a result of an invagination of the pharyngeal membrane. The primitive thyroid originates from the foramen cecum, and descends into the neck via the thyroglossal duct, a tract running from the base of the tongue to the neck. After the thyroid cells have migrated, the thyroglossal duct regresses at approximately week 10. However, in some people, the thyroglossal duct does not regress completely, and parts of or the entire duct remains, giving rise to a thyroglossal cyst.[2]
Patients routinely undergo ultrasound studies prior to undergoing the Sistrunk procedure to determine whether there is a normally functioning thyroid gland in its anatomical position. Thyroid function tests are generally also ordered pre-operatively to determine whether or not the patient is euthyroid. If the patient does not have a functioning thyroid gland, then surgery is not usually performed, in order to minimise the risk of developing hypothyroidism.
Surgical procedure
Thyroglossal cysts are managed by surgical removal. Surgical removal of the thyroglossal cyst is indicated because the cysts are prone to infection, and for cosmetic and aesthetic reasons. In rare instances, thyroglossal cysts may be malignant. This is thought to occur in less than 1% of all cases, and the underlying malignancy is usually papillary thyroid cancer.[2] Thyroglossal cysts are removed by a surgical procedure called the Sistrunk procedure. This operation is named for the surgeon who first described it. Prior to the development of the Sistrunk procedure, thyroglossal cysts were treated merely by incision and drainage, with recurrence being a key issue.
Due to the problems with recurrences, there was a move towards removing the cyst, along with part of the hyoid bone above it. Recurrence rates were lower with this type of operation compared to incision and drainage, but were still quite high. In 1920, Walter Sistrunk described an extended version of the previous operation. The Sistrunk procedure involved removing the cyst and part of the hyoid bone, as well as removing a small core of tissue from the hyoid bone all the way to the foramen cecum, resulting in a much lower rate of recurrence.[1]
How the Sistrunk Procedure is Performed
- A transverse incision is made along the neck is made at the level of the hyoid bone. The incision is approximately 5cm in length.
- The skin and the platysma muscle are reflected to expose the cyst, which is commonly found underneath the raphe which connects the sternohyoid muscles
- The cyst is then dissected away from the surrounding muscles and tissues up to the level of the hyoid bone
- At the hyoid bone, the muscles which attach to the centre of the bone are resected and separated, and then a section of the centre of the hyoid about 2cm is removed together with the cyst and tract.
- From the superior aspect of the hyoid bone up to the level of the foramen cecum, a core of tissue is then removed as needed. The diameter of the core of tissue surrounding the thyroglossal duct is approximately 1cm.
- In the original Sistrunk procedure the foramen cecum was removed, along with part of each genioglossus muscle and the raphe joining the mylohyoid muscles are also removed. This is now only performed as needed depending on the location of the cyst and path of the thyroglossal tract.
- If the tract extended to the tongue base and needed to be removed the opening into the mouth would be closed. Then the genioglossus muscles are sutured, and the tissues at the cut ends of the hyoid bone drawn together with sutures.
- A drain is inserted near the hyoid bone and the skin is closed over it.[3]
Extended Sistrunk Procedure
There are two main limitations of the Sistrunk procedure. Firstly, the procedure does not aim to resect the portion of the thyroglossal duct that lies below the hyoid bone. Secondly, the thyroglossal duct is not a simple, straight tube-like structure. It is often a tortuous structure, particularly between the tongue base and the hyoid bone. In some sections the duct may be incomplete. Furthermore, the duct has several side branches, which may not be resected by the standard Sistrunk procedure. Because the procedure originally described by Sistrunk may not result in complete resection of the entire thyroglossal duct, an extended Sistrunk procedure has been described which aims to surgically remove the entire thyroglossal duct.[4]
For the extended Sistrunk procedure, the skin incision is made lower, usually at the level of the thyroid isthmus. The site of the incision may vary if there are any neck swellings or fistulae that will also need to be resected. Starting at the superior aspect of the thyroid isthmus, a section of tissue which includes both the thyroglossal duct and part of the bordering strap muscles is dissected. The resection continues superiorly towards the hyoid bone, removing the thyroglossal duct and cyst. As with the original Sistrunk procedure, a section of the hyoid bone is removed in the extended procedure. Above the level of the hyoid, the thyroglossal duct and cyst are resected along with a wider core of normal tissue, to ensure that any branches of the thyroglossal duct are also removed. This resection continues until the level of the tongue base; however, the tongue base is ideally not breached by the surgeon. A drain is placed in the neck at the end of the procedure and the wound is closed.[4]
Complications
As with all surgical procedures, there are potential risks and complications associated with both the standard Sistrunk procedure and the extended Sistrunk procedure. Major complications associated with the Sistrunk procedure are rare. Potential major complications include nerve injury, airway injury, thyroglossal cyst recurrence, hypothyroidism, blood transfusion and the development of a haematoma or abscess which may require further surgical intervention.[5]
Minor complications are more common than major complications after surgery. Minor complications are usually related to the wound, including superficial surgical site infections, small abscesses around the sutures, seromas and dehiscence of the wound. These minor complications are associated with very low morbidity and can be easily managed in an outpatient setting.[5]
The risk of developing major complications following the Sistrunk procedure is low for several reasons. The placement of a drain helps to reduce the risk of developing a haematoma and aseptic technique and antibiotic prophylaxis minimises the risk of infection. Furthermore, risk of injury to the airway and major vessels and nerves of the neck can be minimised by employing a meticulous surgical technique and by identifying key anatomical landmarks in order to reduce the risk of inadvertent injury to surrounding structures.[5]
Recurrence
Reported recurrence rates following the Sistrunk procedure are low, between 0 and 8%. In comparison, recurrence rates following incision and drainage of thyroglossal cysts exceeded 50%.[1] One study which has described the use of the extended Sistrunk procedure for primary excision of thyroglossal duct cyst reported a 0% recurrence rate at 3 years follow-up. When the extended Sistrunk procedure is implemented in revision cases, the recurrence rate is 7%.[4]
For more information about thyroglossal duct cyst and Sistrunk procedure click here.
References
[1] Wagner G, Medina JE. Excision of thyroglossal duct cyst: the Sistrunk procedure. Operative Techniques in Otolaryngology (2004); 15: 220-223
[2] Goldsztein H, Khan A, Pereira KD. Thyroglossal duct cyst excision—The Sistrunk procedure. Operative Techniques in Otolaryngology (2009); 20: 256-259.
[3] Sistrunk WE. The surgical treatment of cysts of the thyroglossal duct. Annals of Surgery (1920); 71:121-124.
[4] Ahmed J, Leong A, Jonas N, Grainger J, Hartley B. The extended Sistrunk procedure for the management of thyroglossal duct cysts in children: how we do it. Clinical Otolaryngology (2011); 36:252-279.
[5] Maddalozzo J, Venkatesan TK, Gupta P. Complications associated with the Sistrunk procedure. The Laryngoscope (2001); 111: 119-123.
The post Sistrunk Procedure for Thyroglossal Duct Cyst appeared first on Thyroid Clinic Sydney.